NZ needs a more urgent vaccination plan — with nearly 80% now single-dosed, the majority will support it
- Written by: Rod Jackson, Professor of Epidemiology, University of Auckland

With vaccination rates still too low in Auckland and around Aotearoa New Zealand, and with unexpected cases still showing up, there are few options ahead of today’s government decision[1] on alert levels.
Until there are high levels of immunity, any relaxation of restrictions within Aotearoa when Delta is in the community will dramatically increase the speed at which the virus spreads through the population.
The time has come for a concerted vaccination drive, mandatory vaccination for more workers, and a clear signal that eligible but unvaccinated people will face restricted access to travel and other activities.
With Delta, there is no “herd immunity” — almost everyone who has not been vaccinated will eventually (and sooner rather than later) get infected. Vaccinated people are about 75% less likely than unvaccinated people to develop a COVID infection if exposed, and over 90% less likely to develop severe disease.
In the current Auckland outbreak, only 3% of the more than 1,000 cases were fully vaccinated. There has been only one fully vaccinated patient among the more than 100 hospitalised cases.
With fewer than 10,000 New Zealanders having been infected by COVID-19, unlike most other countries we are completely dependent on high levels of vaccination to provide high levels of immunity.
System overload
Left to its own devices, Delta spreads like wildfire – from 1 person to 6, to 36, to 216, to 1296 and so on – at high speed until there is a high enough vaccination level. This rapid exponential spread is the main threat to health and other essential services.
No hospital system, however many ICU beds per capita, could cope, and no amount of testing would be able to get on top of Delta in an opened-up Aotearoa. Contact tracing systems would be overwhelmed in days.
Without a high vaccination level, increasing hospital capacity or investing in new drugs would be the equivalent of rearranging deck chairs on the Titanic.
Read more: New Zealand cannot abandon its COVID elimination strategy while Māori and Pasifika vaccination rates are too low[2]
Beyond the hospitals, COVID will spread through the unvaccinated 5–11-year-olds at school, who will then infect their teachers, parents and grandparents. Who will be able to care for whom?
Beyond the schools, businesses with clusters of unvaccinated staff will shut down because up to half the unvaccinated infected people will be too sick to work, and up to one in ten could be hospitalised. Asymptomatic infected staff will infect other staff, clients, customers and their families and friends.
Then there is long COVID. A large British study[3] has reported one in three hospitalised COVID cases needed to be readmitted.
In another British study[4], more than half admitted to hospital had long COVID symptoms three months after discharge. Symptoms were worse among those aged under 50, women and those with higher pre-COVID fitness levels.
What are the acceptable costs?
Every national and international health authority has always accepted the only possible sustainable way to deal with COVID is through the development of immunity.
Since the introduction of safe and effective vaccines, every health authority has recommended high levels of vaccination as the only safe and acceptable way to achieve high levels of immunity.
Today, in semi-vaccinated Aotearoa, only two questions are relevant to any plan to open up:
is there a high target vaccination level and what does the target imply about the numbers of infections, hospitalisations, deaths and cases of long COVID considered an “acceptable cost” of opening up?
how does the plan propose to achieve the vaccination target required to meet the “acceptable cost”?
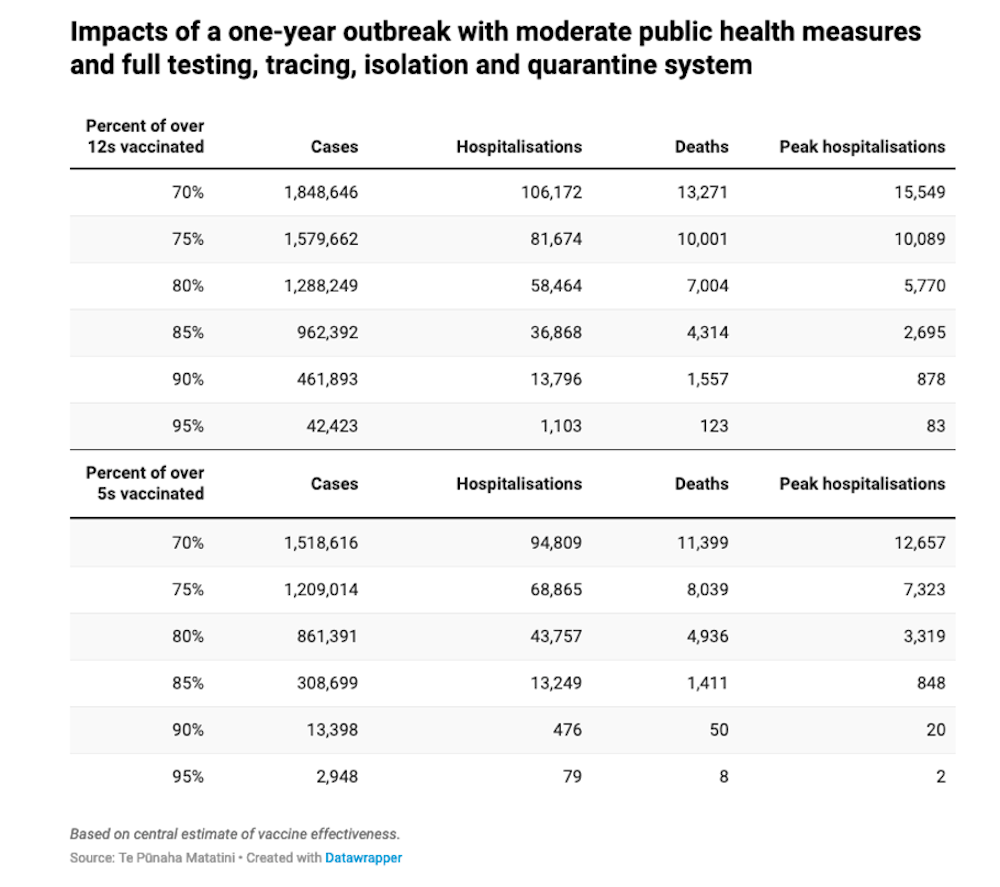
Aotearoa’s most respected COVID-19 modellers, from Te Pūnaha Matatini[5], have provided robust scenarios of the likely impacts of a one-year outbreak at different vaccination levels.
Their modelling assumes moderate public health measures, including a full testing, tracing, isolation and quarantine system. Their predictions are remarkably similar to equivalent predictions from Australian modelling groups (aside from the one used by the federal government).